
Report by Dr. med. R. Kowalski

Endovascular treatment of arterial occlusive disease at the level of the iliac bifurcation is often difficult due to challenging anatomy and the lack of “off-the-shelf” devices. Sometimes we meet the combination of proximal stenosis of the common iliac artery due to calcification or thrombus in combination with distal aneurysmatic degeneration. In these cases the hypogastric artery often cannot be preserved which is associated with buttock claudication or sexual dysfunction.
This is the description of transferring the Covered Endovascular Reconstruction of the Aortic Bifurcation technique (CERAB) to the level of the iliac bifurcation with all of its benefits.
Case Report
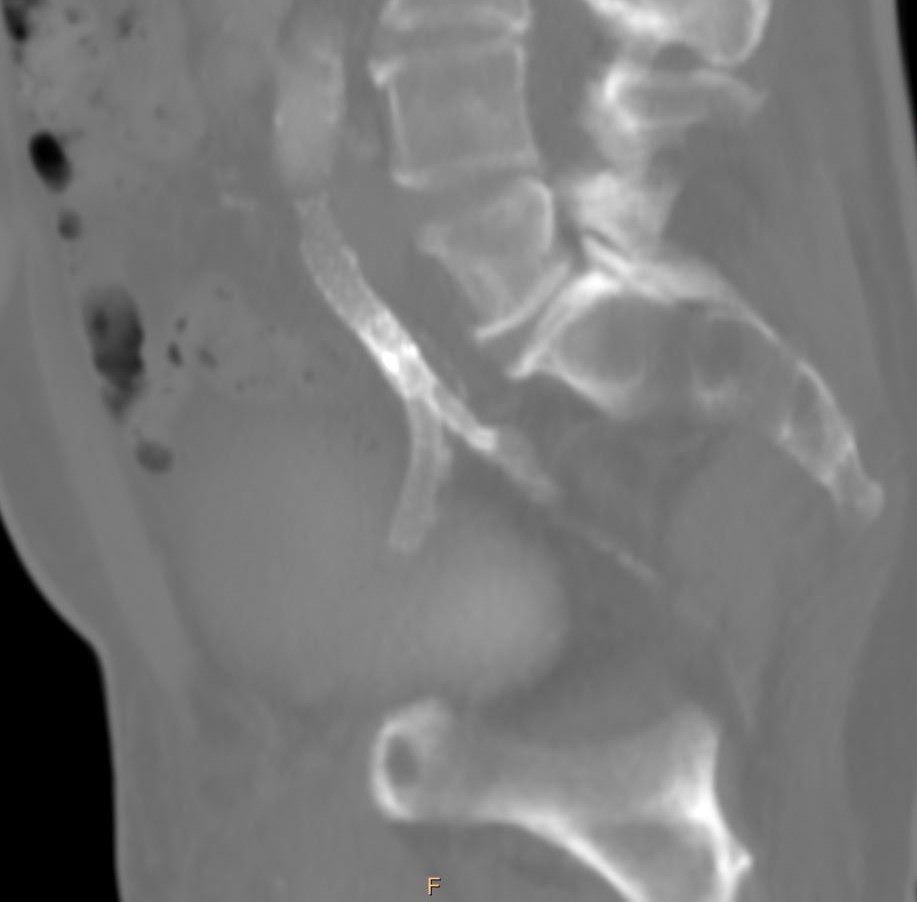
A 69-year old smoker presented with complaints of life-limiting claudication Rutherford class III and a walking capacity of about 10m. The right side ankle-brachial-index (ABI) was significantly abnormal at 0.35. Computed tomography angiography (CTA) revealed a high grade stenosis at the origin of the right common iliac artery ( functional lumen of 2mm) combined with an aneurysmatic degeneration at the level of the iliac bifurcation with high thrombus load resulting in a second high grade stenosis (functional lumen 3mm, aneurysm diameter 24mm).
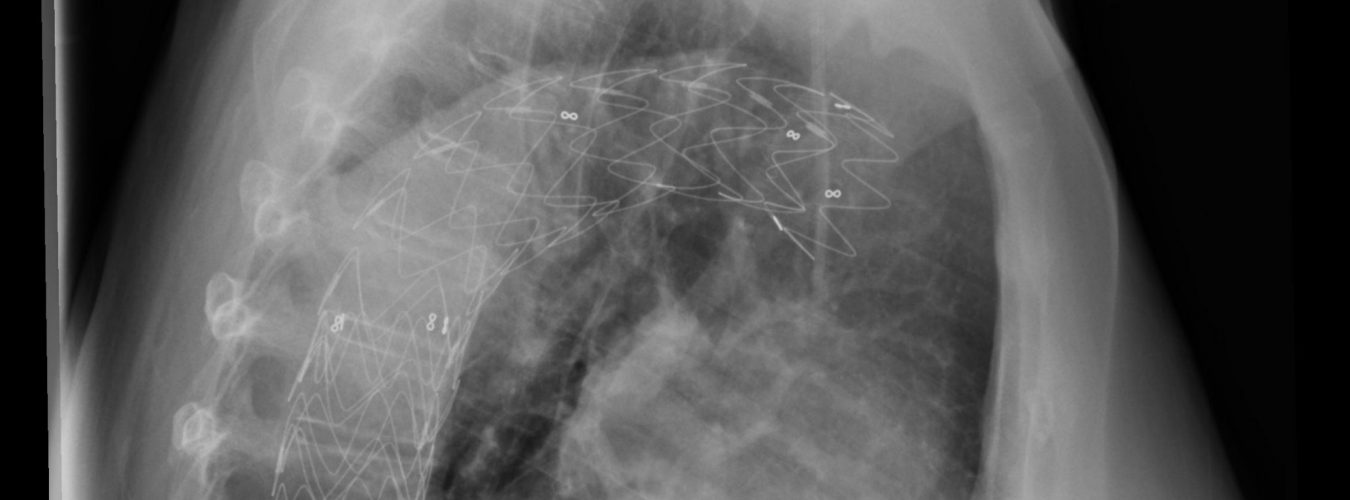
We opted for an endovascular treatment with covered stentgrafts under preservation of the hypogastric artery. A left brachial 6F and a right femoral 7F retrograde approach were established. The lesions were crossed in road map with a .035 guidewire. A 10*57mm covered stent (Bentley BeGraft) was placed at the origin of the right common iliac artery (CIA) under embolic protection of the contralateral CIA with an inflated 10mm balloon and then flared to 13mm in its proximal part. The hypogastric artery (HA) was cannulated from the brachial approach and a 6*39mm covered stent (Bentley BeGraft) was inserted. A second 8*59mm stent (Bentley BeGraft) was inserted from the femoral approach into the external iliac artery (EIA). The proximal part of both stents was placed in sandwich position about 15 mm into the 10mm graft. After simultaneous opening of both stentgrafts their proximal parts were flared to 9 and 7mm. Completion angiography showed a patent EAI and HA with no residual stenosis or endoleak.
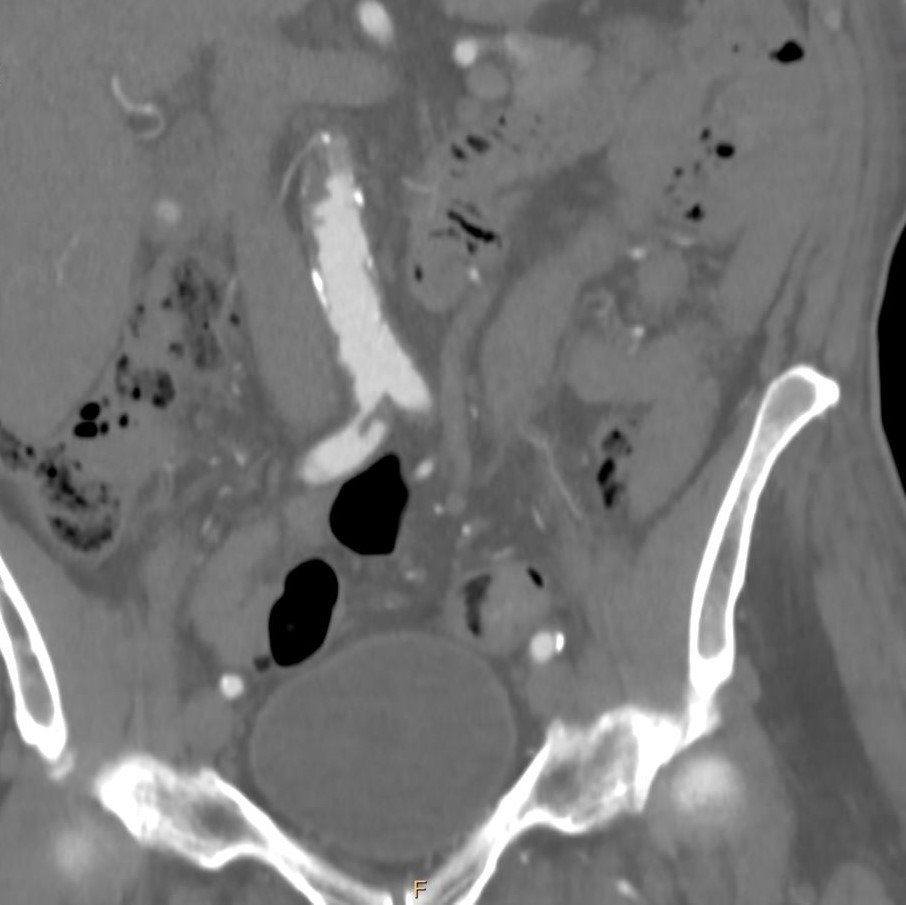
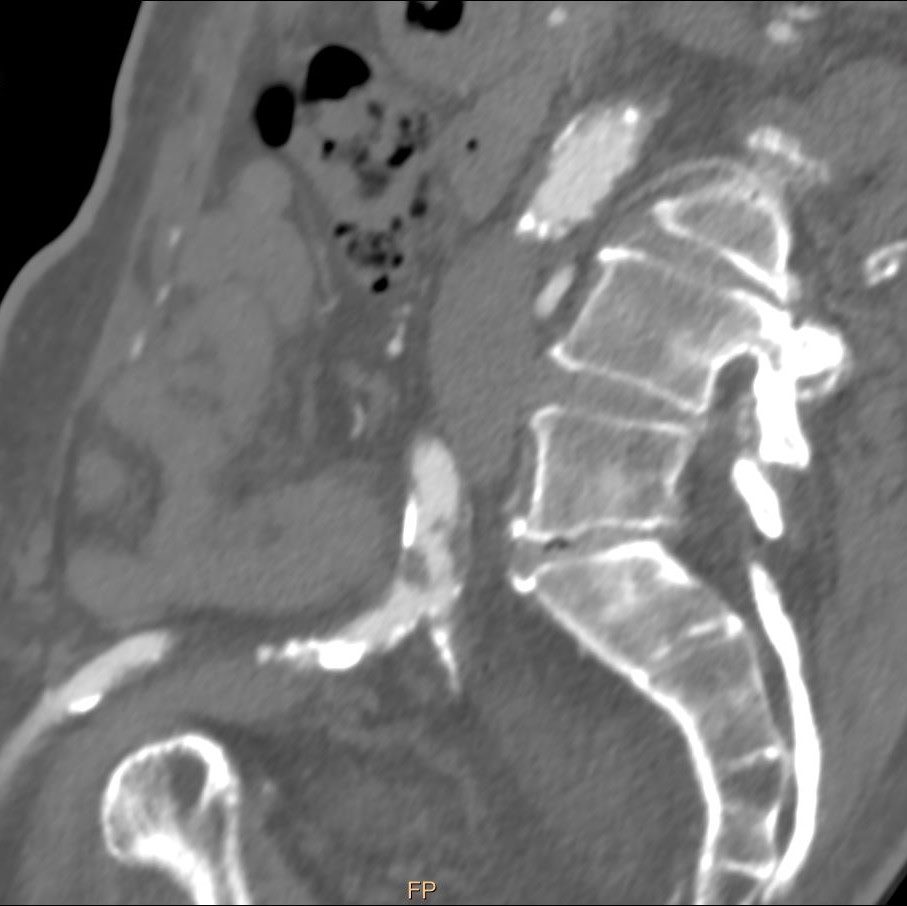
The next day a CT scan was performed and showed a perfect endovascular reconstruction of the iliac bifurcation with no stenosis or endoleak. The patient discharged one day after the procedure on an antiplatelet therapy (acetylsalicylic acid 100 mg daily). The 6 month follow-up showed still patent iliac arteries.