Complex transbrachial iliac and femoral revascularization
History
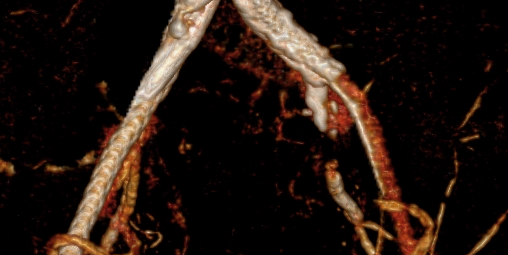
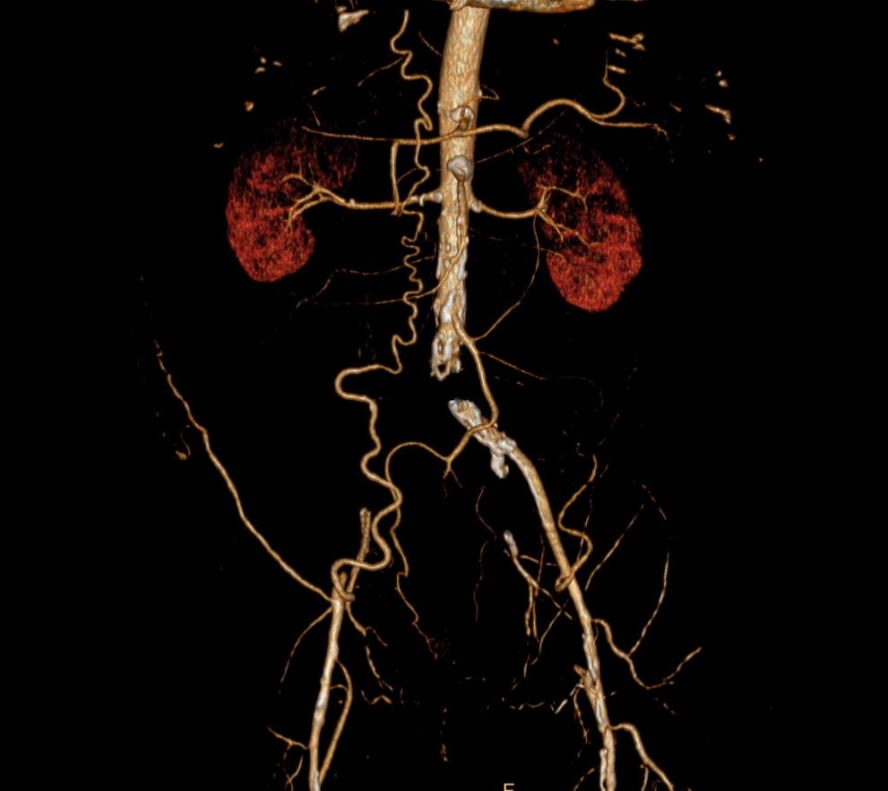
60 year old male with gangrene of the left forefoot and ischemic pain in the right leg . The preoperative CT angiogram showed a total occlusion of the right hypogastric artery, a subtotal occlusion of the left hypogastric artery and an approximately 15cm long CTO of the left superficial artery. In the right hypogastric artery is a 20 year old occluded stent.


Analysis
The next step was the exact analysis of the right iliac occlusion: The stent has been occluded since many years so an intraluminal passage for the guidewire seemed impossible. A 3D endoluminal reconstruction uncovered a small space between the stent and the inner vessel wall.


The strategy
I opted for a left brachial approach due to a better pushability into the iliacs from above and no risk of dissecting the aortic wall during the guidewire passage of the right iliac stent. The approach via the left proximal brachial artery was established and a 100cm 7F sheath inserted and positioned right above the iliac bifurcation.
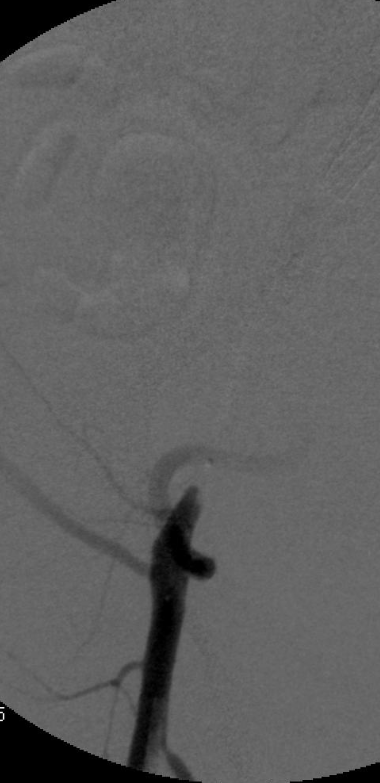
Step by step, the passage of the old stent succeeded with a 0.018 wire and a support catheter and the intraluminal position in the femoral artery was confirmed by angiography.

After insertion of a 7F sheath the guidewire was directed into it and inversed. Due to the high friction between the old stent and the vessel wall it was not possible to pass a balloon or longer sheath behind the occlusion. After exchange to a super stiff guidwire (tensioned thru and thru) we succeded to advance a long sheath from below past the occlusion.
The left iliac high grade stenosis was crossed from proximal.

Then 2 covered stents (8mm Be Graft) were placed in a kissing position and opened simultaneously. The right external iliac was subsequently stented with a Viabahn.

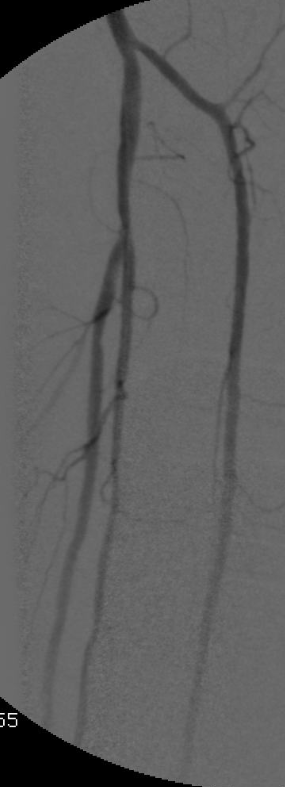
The completion angiogram showed a good result with patent iliacs on both sides.
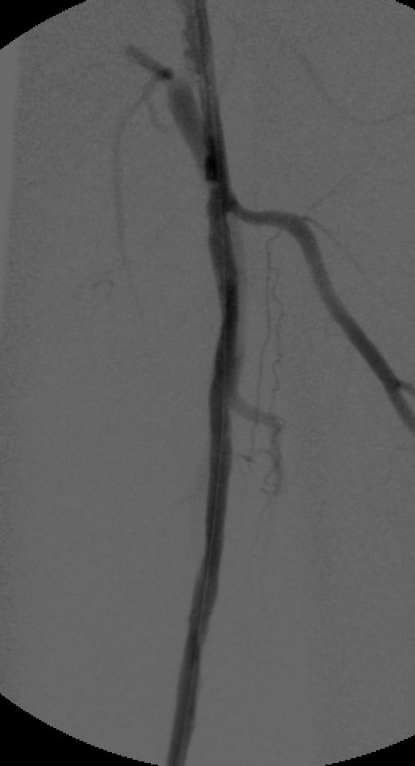
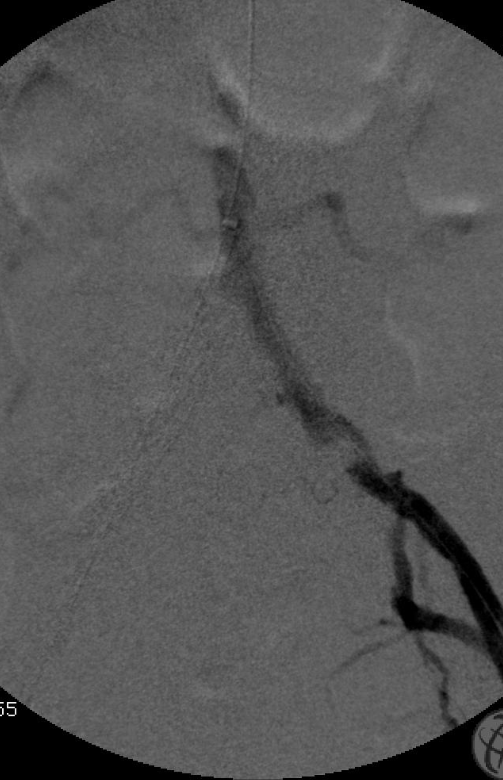
The next step was the crossing of the femoral CTO once again with the help of a 0.018 support catheter. The whole occlusion was then prepared with balloning. Therafter, the entire former occlusion was stented with nitinol stents.
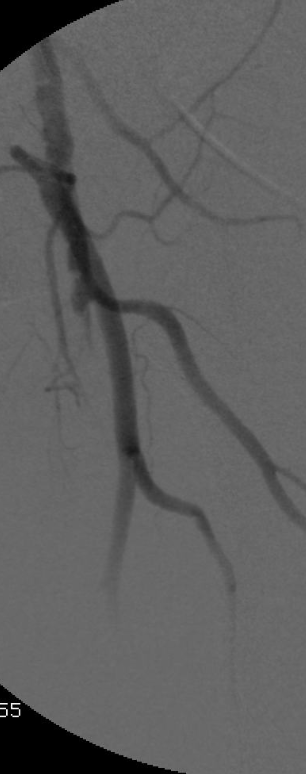


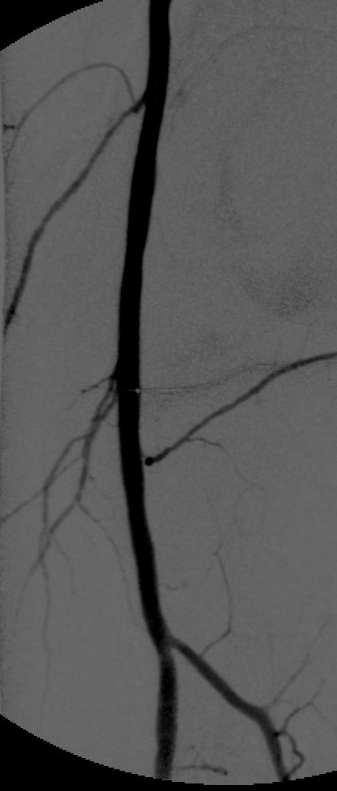
The completion angiogram showed a perfect result with an enormous improvement in peripheral perfusion